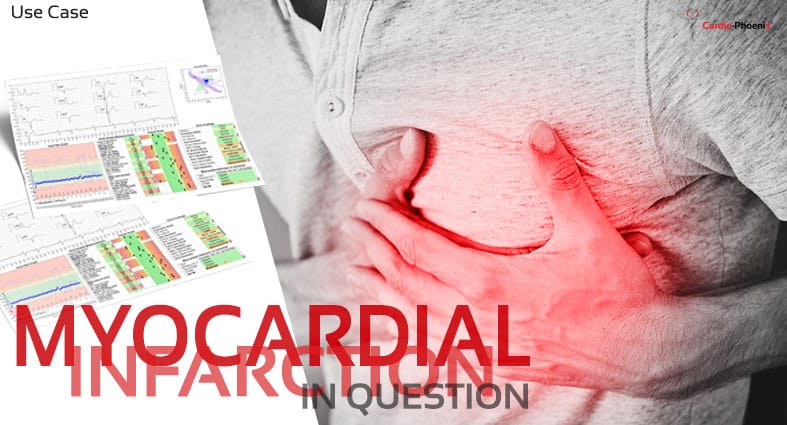

Situation
A symptomatic female patient of 71 years, 161cm, 55kg, was recorded with CHART in primary care because cardiovascular disease is suspected by symptoms.
CHART Report Interpretation
Risk Assessment
• 71-year-old, skinny BMI = 21kg/m2,
• No other information
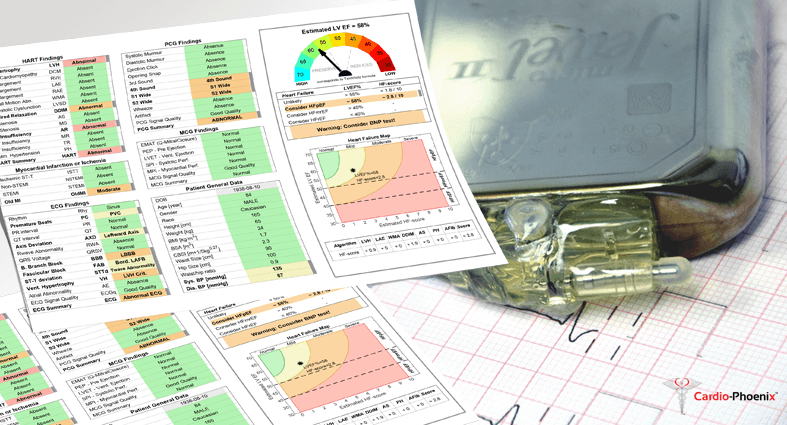
HART-Findings and HF prediction
Abnormal HART summary:
• Abnormal LV hypertrophy
• Mild AV and MV insufficiency
HF prediction:
• Estimated LVEF = 63%
• HF unlikely

ECG
ECG is normal. ECG-based LVH score = 0.
ECG did not indicate mild LVH or MV insufficiency (regurgitation).

PCG
PCG is rather normal, there are only a few borderline sound amplitudes. The heart signal in PCG1 is weak, this is interpreted as passable quality PCG signal. Maybe no murmurs. the opening snap is probably connected to MV insufficiency.

MCG
MCG systolic time intervals show prolonged EMAT (EMAT=93ms), which indicates any abnormality in systolic function.

Decision Support
CHART decision support outcome: Send this patient to cardiology for further diagnosis and treatment with routine priority.

Echocardiographic Results
LV Hypertrophy (LVMI=177g/m2) with preserved systolic function (EF=62%)
MV insufficiency is moderate but needs only pharmacological treatment.
The Aorta wall mildly thickened.
The patient has no heart failure but is classified as borderline HFpEF.
Conclusion
The patient has LVH, which is correctly predicted by HART-findings, but missed by ECG. This becomes the primary decisive finding inpatient referral to cardiology.
The prediction of mild mitral regurgitation was correct, the mild aortic regurgitation is false positive, however, the aorta wall is thickened.
Correct LVEF estimation by CHART.